


 |
市場調查報告書
商品編碼
2066452
抗肥胖藥物:市場佔有率分析、行業趨勢和統計數據以及成長預測(2026-2031 年)Anti-obesity Drugs - Market Share Analysis, Industry Trends & Statistics, Growth Forecasts (2026 - 2031) |
||||||
※ 本網頁內容可能與最新版本有所差異。詳細情況請與我們聯繫。
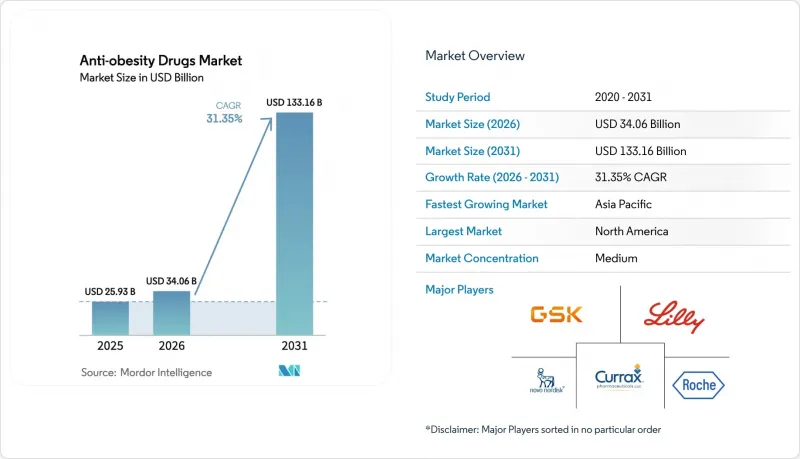
根據 Mordor Intelligence 預測,抗肥胖藥物的市場規模預計將在 2025 年達到 259.3 億美元,在 2026 年達到 340.6 億美元,到 2031 年達到 1331.6 億美元,從 2026 年到 2031 年的複合年成長率為 31.35%。
本報告依作用機轉(周邊脂肪酶抑制劑、中樞擬交感神經藥等)、藥物類型(處方藥和非處方藥)、給藥途徑(口服錠劑和注射)、分銷管道(醫院藥局等)以及地區(北美、歐洲等)進行細分。市場規模和預測均以美元計價。
全球抗肥胖藥物市場趨勢及洞察
心臟代謝併發症發生率的不斷上升,促使人們需要早期藥物治療。
繼美國心臟協會 (AHA) 於 2024 年發布聲明重新定義肥胖之後,循環系統和基層醫療醫生現在將肥胖視為與吸煙同等重要的心血管風險因素。隨後,Semaglutide的 FLOW 試驗顯示,該藥物可使腎臟疾病進展減緩 24%,促使保險公司免除糖尿病腎臟病患者的預先核准要求。預計到 2024 年,美國成年人肥胖率將達到 41.9%,因此臨床指引建議在確診後六個月內開始 GLP-1 療法,而不是在生活方式介入失敗後才開始。企業健康保險計劃已迅速調整其承保範圍以符合這些指南,並增加了 GLP-1 作為第一線治療藥物的處方量。這種縮短的治療路徑目前已在歐洲和日本出現,縮短了從確診到開始藥物治療的時間,並顯著擴大了覆蓋的患者群體。
雇主提供的 GLP-1 保險覆蓋範圍正在迅速擴大,以此作為對沖長期醫療保健成本風險的手段。
2024 年員工福利研究所 (EBRI) 的一項研究發現,為員工提供司美Semaglutide或替魯西帕肽的自保型雇主,在 18 個月內,糖尿病相關保險索賠減少了 12%,心血管住院率減少了 9%,抵消了每年 12,000 至 16,000 美元的藥物費用。因此,2024 年,44% 的美國大型公司將 GLP-1 製劑添加到處方藥清單中,高於 2023 年的 25%。將回扣與持續減重和糖化血紅蛋白 (HbA1c) 降低掛鉤的績效合約正變得越來越普遍,這不僅將風險轉移到了製藥商身上,還推動了藥物依從性計劃的實施。與處方箋一同提供的數位指導,將 12 個月的藥物依從率從 40% 提高到 65%,顯示整合模式可以控制整體成本的成長。加拿大和澳洲也觀察到了類似的趨勢,顯示全球雇主正在效仿這種基於價值的模式來管理慢性病債務。
複雜胜肽類原料藥生產能力瓶頸
固相胜肽合成、高效液相層析純化及冷凍乾燥等製程週期長、產能有限。諾和諾德公司於2024年宣布的60億美元產能擴張計畫以及禮來公司位於印第安納州的53億美元工廠要到2027年才能全面運作,因此預計供應短缺將持續存在。目前全球僅有八家獲得FDA批准的工廠能夠大規模生產GLP-1胜肽,因此,像2024年丹麥供應商發生的火災那樣的突發事件將立即導致全球供應供不應求。為了應對反覆出現的供不應求,歐洲藥品管理局(EMA)已建議處方醫生優先考慮心血管疾病患者,實際上是對治療藥物實施了發行制度。雖然合約研發生產機構(CDMO)的擴建工作正在進行中,但複雜胜肽的法規核准平均需要18至24個月,因此在可預見的未來,供應短缺肯定會持續存在。
細分市場分析
預計到2025年,該細分市場規模將達到131億美元,其中GLP-1單藥療法將佔據38.55%的市場。 2024年12月公佈的來他魯肽(letatorutide)24.2%的減重效果,支持了三重促效劑市場在2031年前將以32.25%的複合年成長率成長的預測。未來五年,隨著臨床醫師尋求克服高劑量GLP-1單藥療法耐受性不足的問題,GIP/GLP-1雙促效劑有望從二線治療轉變為第一線治療。其對升糖素受體的作用預計將進一步減少脂肪量並提高代謝柔軟性,使其對內分泌科醫生、循環系統專家和肝病專家更具吸引力。同時,由於療效有限和安全性方面的權衡,中樞性擬交感神經藥物和脂肪酶抑制劑正逐漸轉向較小的細分市場。
如果證實多促效劑具有心血管和腎臟獲益,保險公司願意承保價格昂貴的此類藥物。目前正在進行的SURMOUNT-5和TRIUMPH-2兩項結果研究正在檢驗這種可能性。鑑於多促效劑具有卓越的減重效果和對合併症的影響,分析師預測,到2031年,它們將佔據抗肥胖藥物市場45%以上的佔有率。安進公司的MariTide和Viking Therapeutics公司的VK2735等新進業者正致力於透過強調獨特的給藥間隔和更佳的胃腸道耐受性來獲取市場佔有率。雖然作用機制的日益複雜性推高了生產成本,但也提高了療效,最終基於價值提高了價格上限。
至2025年,處方藥將佔抗肥胖藥物市場的64.53%,預計到2031年,該領域將以32.85%的複合年成長率成長。 2024年的一項Meta分析顯示,像奧利司他這樣的非處方藥(OTC)僅能將體重減輕效果提高2-3%,這進一步強化了醫生傾向於使用更強效藥物的趨勢。雖然保險可以報銷高達90%的處方藥費用,但非處方藥則完全需要自費,這限制了其使用範圍,使其僅限於經濟條件較好的患者。此外,2024年FDA發布的指南收緊了從處方藥轉向非處方藥的要求,強制要求提供用於慢性病自我篩檢的生物標記,這實際上關閉了消費者使用GLP-1製劑的大門。
未來,能夠帶來兩位數減重或改善心臟代謝終點的藥物預計將繼續作為處方藥的首選。 Rhythm Pharmaceuticals公司的西托美拉諾肽(cetomelanotide)受風險評估和緩解策略(REMS)以及基因檢測的監管,這表明監管機構將如何應對具有複雜安全性特徵的新一代療法。對於非處方藥(OTC)生產商而言,其真正的經濟利益正逐漸縮小,僅限於不會威脅品牌藥業務基礎的輔助產品,例如纖維類食慾抑制劑。
區域分析
預計到2025年,北美將引領抗肥胖藥物市場,佔39.53%的佔有率。這主要得益於北美成人肥胖盛行率超過41%,以及由於聯邦醫療保險D部分(Medicare Part D)覆蓋範圍擴大而新增的1500萬受益人。然而,支付方的成本壓力依然巨大。臨床經濟與評估研究所(ICER)的研究表明,目前GLP-1製劑只有在年價格低於7000美元時才具有成本效益,這導致保險公司要求大幅折扣。加拿大在這方面落後於美國,僅有三個省級公共醫療保險計劃報銷減肥藥,導致患者主要依賴自付費用和雇主提供的保險。墨西哥市場也受到自付費用的限制,但隨著諾和諾德公司於2024年推出低劑量Semaglutide),其價格比美國便宜40%,墨西哥的藥物可及性正在逐步提高。整體而言,北美市場的成長取決於臨床需求與支付方承擔成本能力之間的平衡。
亞太地區預計將成為所有地區中成長最快的地區,到2031年年複合成長率(CAGR)將達到35.21%,這主要得益於中國、日本和印度的法規核准,以及中產階級的快速壯大。中國擁有1.8億肥胖成年人,這是一個巨大的潛在市場,但目前保險覆蓋範圍僅限於第一線城市和私人保險計劃。在日本,保險報銷上限為六個月,且繼續治療需要證明體重減輕5%,這鼓勵了高依從性的治療方法。在印度,價格比品牌注射便宜60%的非專利藥片劑正迅速佔領市場佔有率,顯示其市場推廣主要受成本驅動。在韓國和澳大利亞,國產或進口的GLP-1製劑已獲批准,但公共資金支持的准入標準非常嚴格,限制了其初期推廣。口服製劑和即將上市的生物相似藥對於打入全部區域二、三線城市至關重要。
截至2025年,歐洲約佔抗肥胖藥物市場的25%,但保險報銷標準阻礙了銷售量成長。英國國家健康與臨床最佳化研究所(英國)將Semaglutide的使用限制在體重指數(BMI)≥35 kg/m²的患者,與美國食品藥物管理局(FDA)的標準相比,目標人口減少了60%。在德國,保險報銷設有12個月的上限,之後患者需自費。在法國,保險僅批准用於糖尿病肥胖。 2024年3月,歐洲藥品管理局(EMA)因供不應求發出警告,並推出了優先考慮合併心血管疾病患者的發行方案。波灣合作理事會和非洲仍處於發展中地區,但海灣合作理事會(GCC)成員國出現了一些私人資助的需求。在拉丁美洲,巴西發揮主導作用,25%的人口透過私人保險支付了Semaglutide的費用,但公共醫療體系尚未將其列為優先報銷對象。這些區域差異凸顯了醫療技術評估和預算限制如何影響臨床應用的動機,使其沿著不同的應用曲線發展。
其他好處:
- Excel格式的市場預測(ME)表
- 3個月的分析師支持
目錄
第1章:引言
- 研究假設和市場定義
- 調查範圍
第2章:調查方法
第3章執行摘要
第4章 市場狀況
- 市場概覽
- 市場促進因素
- 心臟和代謝併發症的發生率不斷上升,促使人們更早進行藥物治療。
- 各公司正迅速採用 GLP-1 保險來對沖長期醫療保健成本。
- 突破性的心血管疾病治療結果數據增強了處方醫生的信心,並提高了保險公司的要求。
- 新一代口服小分子 GLP-1 製劑在基層醫療和新興市場的銷售量正在不斷成長。
- 與降低慢性腎臟病風險相關的標籤正在推動多個專業領域的銷售擴張。
- 人工智慧驅動的藥物發現平台正在加速多促效劑研發管線的效率。
- 市場限制因素
- 複雜胜肽類原料藥生產能力瓶頸
- 對罕見眼科不利事件的監管安全監測
- 加強保險公司預算影響管理,克服分階段治療的障礙。
- 在灰色市場銷售藥品正在損害品牌藥的盈利。
- 供應鏈分析
- 監理情勢
- 技術展望
- 波特五力模型
第5章 市場規模與成長預測
- 透過作用機制
- GLP-1受體促效劑
- GIP/GLP-1雙重促效劑
- 三重或多重受體促效劑
- 中樞交感神經興奮劑
- 周邊脂肪酶抑制劑
- 依藥物類型
- 處方藥
- 成藥
- 透過行政途徑
- 注射藥物(每週一次/每月一次)
- 每日口服一次錠劑
- 透過分銷管道
- 醫院藥房
- 零售藥房
- 線上藥局和遠端醫療平台
- 減重診所
- 地區
- 北美洲
- 美國
- 加拿大
- 墨西哥
- 歐洲
- 德國
- 英國
- 法國
- 義大利
- 西班牙
- 其他歐洲國家
- 亞太地區
- 中國
- 日本
- 印度
- 韓國
- 澳洲
- 其他亞太國家
- 中東和非洲
- GCC
- 南非
- 其他中東和非洲國家
- 南美洲
- 巴西
- 阿根廷
- 其他南美國家
- 北美洲
第6章 競爭情勢
- 市場集中度
- 市佔率分析
- 公司簡介
- Altimmune Inc.
- Amgen Inc.
- AstraZeneca plc
- Bayer AG
- Boehringer Ingelheim Intl. GmbH
- Eli Lilly and Company
- F. Hoffmann-La Roche AG
- GSK plc
- Hanmi Pharm. Co., Ltd.
- Innovent Biologics Inc.
- Merck & Co., Inc.
- Novo Nordisk A/S
- Pfizer Inc.
- Rhythm Pharmaceuticals, Inc.
- Structure Therapeutics Inc.
- Takeda Pharmaceutical Co. Ltd
- Teva Pharmaceutical Industries Ltd.
- Viking Therapeutics Inc.
- Zealand Pharma A/S
- Zydus Lifesciences Ltd.
- Currax Pharmaceuticals LLC
第7章 市場機會與未來展望
According to Mordor Intelligence, the anti-obesity drugs market size is projected to be USD 25.93 billion in 2025, USD 34.06 billion in 2026, and reach USD 133.16 billion by 2031, growing at a CAGR of 31.35% from 2026 to 2031.
This report is Segmented by Mechanism of Action (Peripherally Acting Lipase Inhibitors, Centrally Acting Sympathomimetics, and More), Drug Type (Prescription Drugs and OTC Drugs), Route of Administration (Oral Daily Pills and Injectable), Distribution Channel (Hospital Pharmacies, and More), and Geography (North America, Europe, and More). The Market and Forecasts are Provided in Terms of Value (USD).
Global Anti-obesity Drugs Market Trends and Insights
Escalating Cardiometabolic Complications Driving Early Pharmacologic Intervention
Cardiologists and primary-care physicians now regard obesity as a cardiovascular risk factor comparable to smoking, following the American Heart Association's 2024 statement that reclassified the condition. Semaglutide's FLOW trial subsequently showed a 24% reduction in kidney-disease progression, prompting payers to waive prior authorizations for diabetic nephropathy cases. As 41.9% of U.S. adults were living with obesity in 2024, clinical guidelines began recommending GLP-1 initiation within six months of diagnosis rather than after lifestyle failure. Employer health plans quickly aligned benefit designs with these guidelines, fueling a surge in first-line prescriptions. This compressed treatment pathway is now mirrored in Europe and Japan, shrinking the time from diagnosis to pharmacologic therapy and expanding the eligible population at scale.
Rapid Employer Adoption of GLP-1 Coverage as a Hedge Against Long-Term Healthcare Costs
A 2024 Employee Benefit Research Institute analysis found that self-insured employers covering semaglutide or tirzepatide cut diabetes-related claims by 12% and cardiovascular hospitalizations by 9% within 18 months, offsetting annual drug costs in the USD 12,000-16,000 range. As a result, 44% of large U.S. employers added GLP-1s to formularies in 2024 versus 25% in 2023. Outcomes-based contracts that peg rebates to sustained weight loss or HbA1c reduction are spreading, shifting risk to manufacturers and motivating adherence programs. Digital coaching bundled with prescriptions improved 12-month persistence rates from 40% to 65%, demonstrating that integrated models can blunt overall cost growth. Parallel moves in Canada and Australia indicate that employers worldwide are replicating the value-based blueprint to manage chronic-disease liability.
Manufacturing-Capacity Bottlenecks for Complex Peptide APIs
Solid-phase peptide synthesis, HPLC purification, and lyophilization create long cycle times that cap throughput. Novo Nordisk's USD 6 billion capacity build announced in 2024 and Lilly's USD 5.3 billion Indiana plant will not reach full output until 2027, keeping supply constrained. Only eight FDA-approved facilities worldwide can produce GLP-1 peptides at scale, so any disruption, such as the 2024 fire at a Danish supplier, quickly triggers global shortages. The European Medicines Agency responded to recurring deficits by advising prescribers to prioritize cardiovascular patients, effectively rationing therapy. CDMO expansions are underway, but regulatory qualification for complex peptides averages 18-24 months, ensuring that tightness persists in the near term.
Other drivers and restraints analyzed in the detailed report include:
- Breakthrough Cardiovascular-Outcome Data Expanding Prescriber Comfort and Payer Mandates
- Next-Generation Oral Small-Molecule GLP-1s Unlocking Primary-Care and Emerging-Market Volume
- Escalating Payer Budget-Impact Controls and Step-Therapy Barriers
For complete list of drivers and restraints, kindly check the Table Of Contents.
Segment Analysis
The segment generated USD 13.1 billion in 2025, when GLP-1 monotherapies held 38.55% share. Retatrutide's 24.2% weight-loss profile, disclosed in December 2024, underscores why triple-agonists are expected to expand at a 32.25% CAGR through 2031. Over the next five years, dual GIP/GLP-1 agents should migrate from second-line to first-line therapy as clinicians aim to avert tolerability limits seen with higher-dose GLP-1 monotherapy. The addition of glucagon-receptor activity promises incremental fat-mass reduction and metabolic flexibility, broadening appeal to endocrine, cardiology, and hepatology specialists. Meanwhile, centrally acting sympathomimetics and lipase inhibitors are sliding toward low-volume niches, constrained by modest efficacy and safety trade-offs.
Payers are signaling willingness to reimburse premium-priced multi-agonists if cardiovascular or renal benefits materialize, a possibility under investigation in ongoing SURMOUNT-5 and TRIUMPH-2 outcome studies. Given superior weight loss and comorbidity impact, analysts expect multi-agonists to exceed 45% of the anti-obesity drugs market by 2031. New entrants such as Amgen's MariTide and Viking Therapeutics' VK2735 target differentiated dosing intervals or improved GI tolerability to carve share. The escalation in mechanism complexity heightens manufacturing cost but also raises efficacy and, by extension, value-based price ceilings.
Prescription products represented 64.53% of the anti-obesity drugs market in 2025, and the cohort is on track for a 32.85% CAGR through 2031. Over-the-counter alternatives like orlistat delivered only 2-3% incremental weight loss in 2024 meta-analyses, reinforcing prescriber reliance on higher-efficacy options. Payer formularies absorb up to 90% of prescription costs for eligible patients, whereas OTC products are fully out-of-pocket, limiting their reach to affluent self-payers. FDA guidance in 2024 also tightened the path for Rx-to-OTC switches by requiring biomarkers for chronic-disease self-selection, effectively closing the door to consumerized GLP-1s.
Going forward, prescription status will likely remain the default for any agent demonstrating double-digit weight loss or cardiometabolic endpoints. Rhythm Pharmaceuticals' setmelanotide, gated by a REMS and genetic testing, signals how regulators may handle next-generation therapies with complex safety profiles. For OTC players, the viable economic niche is slimming down to adjunctive products such as fiber-based appetite suppressants, which do not threaten branded franchises.
Geography Analysis
North America dominated with 39.53% of the anti-obesity drugs market in 2025, buoyed by obesity prevalence surpassing 41% of adults and expanding Medicare Part D coverage that raised the eligible pool by 15 million beneficiaries. Still, payer cost pressures remain acute; the Institute for Clinical and Economic Review deemed current GLP-1 prices cost-effective only below USD 7,000 annually, prompting insurers to demand steep rebates. Canada lags the United States, as public plans in only three provinces reimburse obesity drugs, creating reliance on private pay or employer coverage. Mexico's market is limited by out-of-pocket spend, but Novo Nordisk's lower-dose semaglutide at 40% below U.S. pricing began expanding access in 2024. Overall, North American growth will hinge on balancing clinical demand with payer affordability thresholds.
Asia-Pacific is forecast to post a 35.21% CAGR through 2031, the fastest among all regions, aided by regulatory approvals in China, Japan, and India alongside rapid middle-class expansion. China's 180 million adults with obesity constitute a massive addressable population, though reimbursement is confined to tier-1 cities and private plans. Japan's six-month reimbursement cap mandates demonstrable 5% weight loss for continuation, incentivizing high-adherence regimens. In India, a generic tablet priced 60% below the branded injectable quickly captured share, signaling cost-sensitive adoption pathways. South Korea and Australia approved local or imported GLP-1s but apply stringent BMI thresholds for publicly funded access, tempering early uptake. Oral formulations and forthcoming biosimilars are essential to unlocking second- and third-tier city penetration across the region.
Europe controlled roughly 25% of the anti-obesity drugs market in 2025, yet reimbursement gatekeeping restrains volume growth. NICE restricts semaglutide to BMI >= 35 kg/m2, shrinking the eligible population by 60% relative to FDA criteria. Germany enforces a 12-month reimbursement cap, requiring self-pay thereafter, while France approves coverage only for diabetic obesity. Shortages prompted an EMA alert in March 2024, leading to rationing protocols prioritizing cardiovascular co-morbid patients. Middle East and Africa remain nascent but show pockets of private-pay demand in Gulf Cooperation Council states. Latin America is led by Brazil, where private insurance, covering 25% of residents, funds semaglutide, but public systems have not prioritized coverage. Overall regional variability highlights how health-technology assessments and budget constraints filter clinical enthusiasm into disparate adoption curves.
- Altimmune Inc.
- Amgen
- AstraZeneca
- Bayer
- Boehringer Ingelheim Intl. GmbH
- Eli Lilly and Company
- Roche
- GlaxoSmithKline
- Hanmi Pharm. Co., Ltd.
- Innovent Biologics Inc.
- Merck
- Novo Nordisk
- Pfizer
- Rhythm Pharmaceuticals, Inc.
- Structure Therapeutics Inc.
- Takeda Pharmaceuticals
- Teva Pharmaceutical Industries
- Viking Therapeutics Inc.
- Zealand Pharma
- Zydus Lifesciences Ltd.
- Currax Pharmaceuticals
Additional Benefits:
- The market estimate (ME) sheet in Excel format
- 3 months of analyst support
TABLE OF CONTENTS
1 Introduction
- 1.1 Study Assumptions & Market Definition
- 1.2 Scope of the Study
2 Research Methodology
3 Executive Summary
4 Market Landscape
- 4.1 Market Overview
- 4.2 Market Drivers
- 4.2.1 Escalating cardiometabolic complications driving early pharmacologic intervention
- 4.2.2 Rapid employer adoption of GLP-1 coverage as a hedge against long-term healthcare costs
- 4.2.3 Breakthrough cardiovascular-outcome data expanding prescriber comfort and payer mandates
- 4.2.4 Next-generation oral small-molecule GLP-1s unlocking primary-care and emerging-market volume
- 4.2.5 Chronic kidney-disease risk-reduction labeling creating multi-specialty pull-through
- 4.2.6 AI-enabled drug-discovery platforms accelerating multi-agonist pipeline productivity
- 4.3 Market Restraints
- 4.3.1 Manufacturing-capacity bottlenecks for complex peptide APIs
- 4.3.2 Regulatory safety surveillance around rare ophthalmic adverse events
- 4.3.3 Escalating payer budget-impact controls and step-therapy barriers
- 4.3.4 Grey-market compounding eroding branded-drug economics
- 4.4 Supply-Chain Analysis
- 4.5 Regulatory Landscape
- 4.6 Technological Outlook
- 4.7 Porter's Five Forces
- 4.7.1 Threat of New Entrants
- 4.7.2 Bargaining Power of Buyers
- 4.7.3 Bargaining Power of Suppliers
- 4.7.4 Threat of Substitute Products
- 4.7.5 Intensity of Competitive Rivalry
5 Market Size & Growth Forecasts (Value, USD)
- 5.1 By Mechanism of Action
- 5.1.1 GLP-1 Receptor Agonists
- 5.1.2 Dual GIP/GLP-1 Agonists
- 5.1.3 Triple or Multi-Receptor Agonists
- 5.1.4 Centrally Acting Sympathomimetics
- 5.1.5 Peripherally Acting Lipase Inhibitors
- 5.2 By Drug Type
- 5.2.1 Prescription Drugs
- 5.2.2 OTC Drugs
- 5.3 By Route of Administration
- 5.3.1 Injectable (Weekly / Monthly)
- 5.3.2 Oral Daily Pills
- 5.4 By Distribution Channel
- 5.4.1 Hospital Pharmacies
- 5.4.2 Retail Pharmacies
- 5.4.3 Online Pharmacies & Tele-health Platforms
- 5.4.4 Weight-Loss Clinics
- 5.5 Geography
- 5.5.1 North America
- 5.5.1.1 United States
- 5.5.1.2 Canada
- 5.5.1.3 Mexico
- 5.5.2 Europe
- 5.5.2.1 Germany
- 5.5.2.2 United Kingdom
- 5.5.2.3 France
- 5.5.2.4 Italy
- 5.5.2.5 Spain
- 5.5.2.6 Rest of Europe
- 5.5.3 Asia-Pacific
- 5.5.3.1 China
- 5.5.3.2 Japan
- 5.5.3.3 India
- 5.5.3.4 South Korea
- 5.5.3.5 Australia
- 5.5.3.6 Rest of Asia-Pacific
- 5.5.4 Middle East and Africa
- 5.5.4.1 GCC
- 5.5.4.2 South Africa
- 5.5.4.3 Rest of Middle East and Africa
- 5.5.5 South America
- 5.5.5.1 Brazil
- 5.5.5.2 Argentina
- 5.5.5.3 Rest of South America
- 5.5.1 North America
6 Competitive Landscape
- 6.1 Market Concentration
- 6.2 Market Share Analysis
- 6.3 Company Profiles (includes Global level Overview, Market level overview, Core Segments, Financials as available, Strategic Information, Market Rank/Share for key companies, Products & Services, and Recent Developments)
- 6.3.1 Altimmune Inc.
- 6.3.2 Amgen Inc.
- 6.3.3 AstraZeneca plc
- 6.3.4 Bayer AG
- 6.3.5 Boehringer Ingelheim Intl. GmbH
- 6.3.6 Eli Lilly and Company
- 6.3.7 F. Hoffmann-La Roche AG
- 6.3.8 GSK plc
- 6.3.9 Hanmi Pharm. Co., Ltd.
- 6.3.10 Innovent Biologics Inc.
- 6.3.11 Merck & Co., Inc.
- 6.3.12 Novo Nordisk A/S
- 6.3.13 Pfizer Inc.
- 6.3.14 Rhythm Pharmaceuticals, Inc.
- 6.3.15 Structure Therapeutics Inc.
- 6.3.16 Takeda Pharmaceutical Co. Ltd
- 6.3.17 Teva Pharmaceutical Industries Ltd.
- 6.3.18 Viking Therapeutics Inc.
- 6.3.19 Zealand Pharma A/S
- 6.3.20 Zydus Lifesciences Ltd.
- 6.3.21 Currax Pharmaceuticals LLC
7 Market Opportunities & Future Outlook
- 7.1 White-space & Unmet-Need Assessment
 抗肥胖藥物市場:依產品類型、劑型、給藥途徑及最終用戶分類-2026-2032年全球市場預測
抗肥胖藥物市場:依產品類型、劑型、給藥途徑及最終用戶分類-2026-2032年全球市場預測 抗肥胖藥物市場:依作用機制、處方藥/非處方藥及地區分類。
抗肥胖藥物市場:依作用機制、處方藥/非處方藥及地區分類。 抗肥胖藥物市場分析及至2035年預測:類型、產品、服務、技術、組件、應用、劑型、最終用戶、設備、模式
抗肥胖藥物市場分析及至2035年預測:類型、產品、服務、技術、組件、應用、劑型、最終用戶、設備、模式 抗肥胖藥物市場規模、佔有率、趨勢及預測(依藥物類別、藥物類型、通路及地區分類,2026-2034年)
抗肥胖藥物市場規模、佔有率、趨勢及預測(依藥物類別、藥物類型、通路及地區分類,2026-2034年) 抗肥胖藥物市場-全球產業規模、佔有率、趨勢、機會與預測:按作用機制、藥物類型、地區和競爭格局分類,2021-2031年
抗肥胖藥物市場-全球產業規模、佔有率、趨勢、機會與預測:按作用機制、藥物類型、地區和競爭格局分類,2021-2031年 抗肥胖藥物市場-2026-2031年預測
抗肥胖藥物市場-2026-2031年預測 抗肥胖藥市場:2035年前的產業趨勢和全球預測 - 各分子類型,-+化合物,各作用機制,各促效劑類型,各作用途徑,各給藥途徑,各地區,預測銷售額,主要企業
抗肥胖藥市場:2035年前的產業趨勢和全球預測 - 各分子類型,-+化合物,各作用機制,各促效劑類型,各作用途徑,各給藥途徑,各地區,預測銷售額,主要企業 抗肥胖藥的全球市場:治療類型·藥物類型·作用機制·給藥途徑·通路·各地區 (~2035年)
抗肥胖藥的全球市場:治療類型·藥物類型·作用機制·給藥途徑·通路·各地區 (~2035年) 2021 - 2031 年抗肥胖藥物市場規模及預測、全球及地區佔有率、趨勢及成長機會分析報告,涵蓋:按類型、藥物類別、應用、給藥途徑、配銷通路和地理分類
2021 - 2031 年抗肥胖藥物市場規模及預測、全球及地區佔有率、趨勢及成長機會分析報告,涵蓋:按類型、藥物類別、應用、給藥途徑、配銷通路和地理分類 抗肥胖藥物市場規模、佔有率、成長分析(按藥物類型、作用、劑量和地區分類)- 產業預測,2025 年至 2032 年
抗肥胖藥物市場規模、佔有率、成長分析(按藥物類型、作用、劑量和地區分類)- 產業預測,2025 年至 2032 年